(Cross posted from the ThinkGP blog)
Many years ago, coming to general practice from an emergency medicine background, I sat down with a group of trainee GPs. We started to talk about what we would see in general practice. I’d been working as a locum in general practice for a year and I thought I knew everything. ‘Coughs and colds are the bulk of the work’, I confidently declared. Those older and wiser than me set me straight, and told me that general practice is all about depression and anxiety and that it’ll be a rare consult where these won’t play a role. They were wise words then and now, so let’s talk about major depression in general practice.
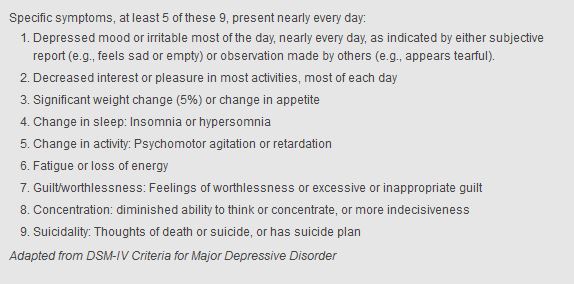
The books would describe major depression as a subjective diagnosis which depends on reported symptoms rather than objective signs. There are cardinal symptoms of depression, rather than signs. Five or more of the symptoms below, present most of the time nearly every day for at least two consecutive weeks. Depressed mood or loss of interest or pleasure must be present. The symptoms cause substantial distress or impair function, and they are not better explained by substance abuse or a general medical problem. They are over and above what the GP thinks would be normal given the patient’s situation.
The GP who relies on books alone will be well read… and alone. Listen to the patient! It’s a mood disorder. How do they feel? How do they make you feel? Clinical gestalt is the theory that healthcare practitioners actively organise clinical perceptions into coherent construct wholes, or simply put, how experienced GPs can spot depression a mile off. Listen to your gut. Countertransference can be a powerful tool to show you where you need to go. We’ll come back to the Art of General Practice later. Experienced GPs can’t be everywhere, and so we need some other ways to screen for depression.
Enter the rating scales for depression. They read like the alphabet – PHQ-9, BDI, HDRS. They can be used for screening and measurement of progress. Perhaps only 50 percent of patients with major depression are identified without screening [1]. Patients may not volunteer depressive symptoms without direct questioning for many reasons including fear of stigma, a belief that depression is not a matter for primary care, or a belief that depression isn’t a “real” illness but rather a personal flaw, as well as concerns about confidentiality and antidepressant medication [2].
In Australian general practice, we use the K10 and the DASS21 or 42. These are validated, easy to administer, reproducible, and recognised as part of the Mental Health Care Planning process. This enables patients with diagnosed depression to obtain a Medicare rebate for psychological therapy with a psychologist. American studies show patients are scared of psychiatric referral. Australian GPs are also scared of psychiatric referral, as it can be hard work to access private psychiatry. MBS item number 291 comes to the rescue and many psychiatrists will use this. They also know that depression masquerades as a variety of somatic symptoms. Untreated depression is associated with decreased quality of life and increased mortality. Depression can be successfully treated and treatment is effective. The earlier the better!
I recommend non-pharmacological treatment regularly. Exercise, diet, psychotherapy, GP counselling, reducing drug and alcohol use, getting more and better sleep are all options. These take time and effort, both from the patient and the GP. Remember, your time and presence are important to your patients. Ten minutes of education on diet and exercise can be worth months of medication and the effect can be long-lasting. Red flags include significant physical signs (weight loss is the big one in my opinion) or symptoms such as suicidality or psychosis on mental state examination.
Depression is not just a chemical imbalance. No pill can defeat the entirety of the patient’s life and circumstances pushing them in the wrong direction. The good GP will consider the patient in their environment and have an awareness of the social determinants of depression. Personality disorders, illicit drug use, and past abuse can lead to poor life choices and situations. Think about these before printing out a script.
When selecting an antidepressant, ask the patient what they’ve been on before. Ask about expectations and experiences and how they define success or failure. I tend to use medications that I’m familiar with and can then counsel patients accordingly. I find SSRIs to be an appropriate first line treatment. The side effects that concern my patients are anticholinergic (dry mouth), sexual (decreased libido and prolonged time to orgasm/ejaculation – so common that medications are now marketed for this purpose alone), and changes in sleep (too wakeful and agitated or too sleepy and hungover). I combat these with the advice to drink plenty of water and to time your medication according to how it makes you feel.
Traditionally, antidepressants are taken in the morning, but for those with a significant anxiety component, evening dosing is best. Trial and error will determine the optimal time for a good night’s sleep with no morning hangover. Sexual issues often require a change in medication. The newer medications promise fewer sexual issues, but often an older alternative can achieve the same goals at much lower cost.
The literature tells us the most resistant symptoms to treatment are insomnia, followed by sad mood, and decreased concentration. Depression is more likely to reoccur if these symptoms are persistent. I find that fatigue, anhedonia, guilt, worthlessness, and poor concentration are the hardest symptoms to treat successfully. It can be a long road for the patient (and the GP) back to wellness, and it can be hard to stick with treatment over time.
GPs have used many strategies to improve treatment adherence and all of us will remember pre-contemplators from our studies. We all get frustrated when patients don’t take our advice but providing information and warning of future consequences doesn’t always work. However, a solution is in clear sight. GPs have a fantastic and privileged therapeutic relationship with their patients, and can use this to capitalise on the essential window of time before you deliver your medical advice. This “privileged moment for change” prepares people to be receptive to a message before they experience it. Robert Cialdini has coined the term ‘pre-suasion’ to describe this. The therapeutic relationship allows pre-suasion, and therapeutic change can then be addressed, with consideration of the patient’s motivation, opportunity, and ability.
You can see the themes above of time and a relationship as potent therapy for the management of major depressive disorder in general practice. The initial clinical gestalt and the ongoing therapeutic relationship can be powerful tools for change. Depression is subjective and has been part of the human condition throughout history. This gives us all we need to move forward. Focus on the whole person sitting in front of you. Give them your time and expertise, be thorough, be kind, and be present. It therefore seems fitting to end with the words of a doctor from another time:
“The three grand essentials of happiness are: Something to do, someone to love, and something to hope for.”
Alexander Chalmers (29 March 1759 – 29 December 1834)
If you are worried about depression, anxiety, or have any other mental health concerns, reach out:
ACIS 131465 (South Australia – Acute Crisis Intervention Service)
Your GP at Partridge Street General Practice
Dr Gareth Boucher
Dr Ali Waddell
Dr Emmy Bauer
Dr Nick Mouktaroudis
Dr Nick Tellis
Beyond Blue & Beyond Blue New Access (free mental health coaching)

Reach Out
References
- Mitchell AJ, Vaze A, Rao S. Clinical diagnosis of depression in primary care: a meta-analysis. Lancet. 2009 Aug;374(9690):609-19
- Bell RA, Franks P, Duberstein PR, Epstein RM, Feldman MD, Fernandez y Garcia E, Kravitz RL. Suffering in silence: reasons for not disclosing depression in primary care. Ann Fam Med. 2011 Sep;9(5):439-46.
Thanks to Klarem for the beautiful picture above, Marcia Vernon for the Beyond Blue link, and the guys at ThinkGP for their editing and help.
Trackbacks/Pingbacks